Using Ventilation Systems to Limit the Spread of Airborne Infections




Recirculated Air (Return)
Recirculated or return air — air that is routed back to the AHUs before it is filtered, conditioned, and returned to the space — is a very important part of the ventilation air in a hospital. Recirculation by in-room units is not allowed in most of the critical spaces within a hospital, and, therefore, units like fan coil units, VRV units, chilled beams, induction units, etc. are not allowed within critical spaces.
The quality of this recirculated air is very important in maintaining a ventilation system’s effectiveness within health care settings. This air is also important to minimize hospitals’ energy use so that these facilities can meet ASHRAE 90.1 energy guidelines. During the pandemic, air recirculated from areas that housed cohorts of infected COVID-19 patients was not allowed to return to the AHUs that served other areas. Many facilities added HEPA fan units to intercept the return path within the ductwork and discharged the return air outside of the hospital. In those cases, the return air became exhaust (Figure 2).
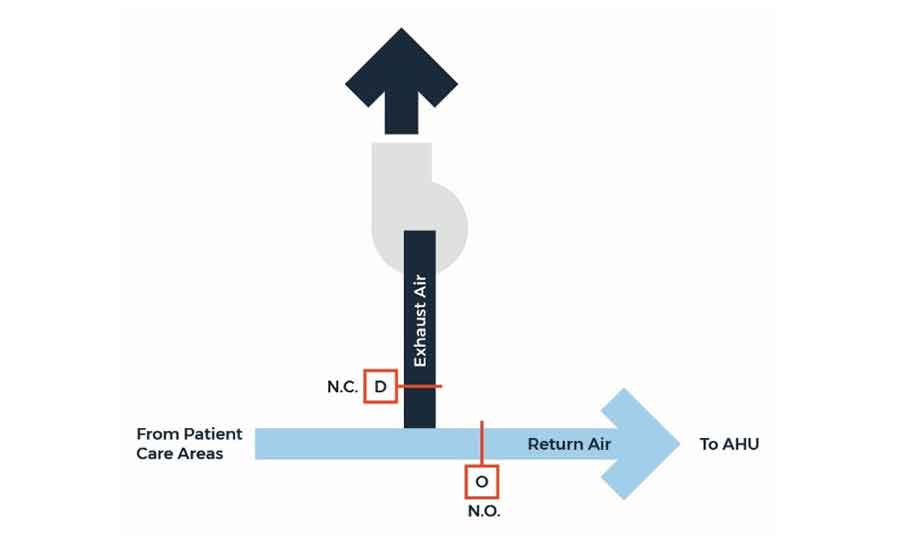
FIGURE 2. A purge mode system.
Pandemic Ventilation Design
The ventilation design for hospitals will need to be revisited to ensure these systems may be easily modified to meet future pandemic requirements. There are some recommendations that can help these systems prepare for future pandemic occurrences, such as:
- Return air tracking boxes paired with a supply box to allow room control of pressurization. This will allow an easier modification to negative pressure for the standard patient rooms.
- Pandemic exhaust fans dedicated to floors or wings by utilizing return air pathways to each floor. This will allow floors to be converted to negative isolation floors
(see Diagram 1). - Cooling coils will be sized to handle 100% outdoor air at peak loads. This will allow the AHUs to operate in 100% outside air mode year-round.
- Designing an exhaust purge mode that is able to flush the hospital floor by floor. The system will need to have the ability to activate an exhaust fan that is only activated during the purge mode.
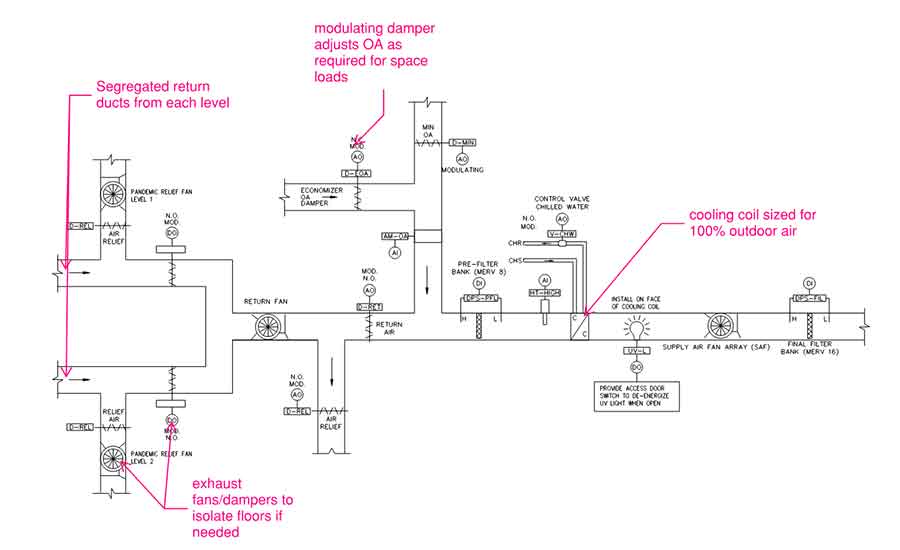
DIAGRAM 1. An air-handling unit control diagram.
Conclusion
Ventilation systems on their own are not the end-all, be-all engineering solution to minimize the airborne transmission of viruses like COVID-19. Ventilation systems are most helpful when combined with other hospital airflow systems, such as HEPA air filtration; ultraviolet germicidal irradiation (UVGI); and other means of deactivating viruses, bacteria, and other microorganisms. Efficacy of the HEPA filtration and UVGI on the COVID-19 virus is still under investigation, but based on their effects on other viruses, it can be inferred that they will impact the virus’s activity in an airflow system. Care must be taken to ensure the modification of one part of a ventilation system does not negatively affect the overall air system’s performance. One thing is certain: Designers cannot design ventilation systems without at least considering future pandemic occurrences.
Images courtesy of WSP
|
Gary Hamilton, is a senior vice president and health care practice lead at WSP. He is a licensed professional engineer in the U.S. as well as in Europe and has more than 23 years of experience in the design and analysis of HVAC systems for a variety of market sectors but with special focus on health care facilities. He has written more than 24 articles in multiple health care and engineering publications. He is also a seasoned presenter and has presented across the country and globally. |
